Support
Support FINE-TUNE
FINE-TUNE ORDER SERVICES
ORDER SERVICES PRODUCT SHOP
PRODUCT SHOP 1-866-834-7925
1-866-834-7925
Top 5 Freehand Implant Mistakes and How to Avoid Them with Guided Surgery
Dental implant placement is a delicate procedure where precision matters. Yet, many clinicians still perform implants freehand, relying solely on clinical experience and tactile feedback. While this technique can work for seasoned surgeons, it often carries a higher risk of errors that can compromise outcomes.
In this article, we’ll explore the top 5 freehand implant mistakes, explain why they happen, and how guided surgery solutions can dramatically reduce these risks
What is Freehand Implant Placement?
Freehand implantology refers to placing implants without the use of a surgical guide or digital planning tools. The clinician determines angulation, depth, and position visually and manually, based on clinical assessment and radiographic interpretation.
While this method offers flexibility, it inherently lacks the precision of CBCT-based implant planning and surgical guides.

Top 5 Freehand Implant Mistakes
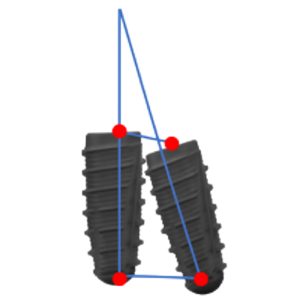
1. Improper Implant Angulation
Freehand placement often results in implants being angled incorrectly, leading to:
- Prosthetic complications
- Poor load distribution
- Esthetic failures
A study published in The International Journal of Oral & Maxillofacial Implants found that angular deviations of up to 13° are common in freehand placements (Van Assche et al., 2012).
Solution:
Utilizing digital dental design services and custom surgical guides ensures optimal angulation, minimizing the risk of esthetic or functional compromise.
Angular deviations with guided surgery are typically 2.5–4.0°, which is 70–80% reduction in deviation
2. Incorrect Implant Depth
Placing implants too shallow or too deep can result in:
- Bone dehiscence
- Peri-implantitis
- Prosthetic misfit
According to Bornstein et al. (2014), vertical deviations in freehand implant placement can exceed 1.5mm, significantly impacting restorative outcomes.
Solution:
Full-arch guided surgery workflows control implant depth with precision, guided by pre-planned CBCT data and digital designs.
Vertical deviations typically between 0.6–1.0 mm, reducing depth errors by over 40%, ensuring optimal implant positioning in relation to soft tissue and restorative components.

3. Inadequate Inter-Implant Distance
Insufficient spacing between implants or between implants and adjacent teeth can:
- Compromise blood supply to adjacent teeth and implant
- Affect soft tissue stability
- Hinder prosthetic design
Research by D’haese et al. (2012) emphasizes that freehand techniques often lead to spacing deviation at implant neck can exceed 1.5–2.0 mm, increasing the risk of implant failure.
Solution:
Surgical guides designed through prosthetic-driven planning ensure proper spacing, preserving bone and soft tissue architecture.
Guided Surgery minimizes deviation at neck to approximately 0.9–1.2 mm, maintaining restorative-driven spacing, improving esthetics, hygiene access, and prosthetic integrity.
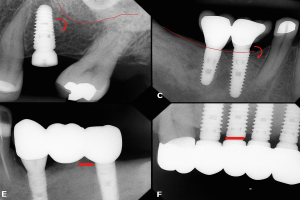
4. Lingual or Buccal Perforations
Lack of visibility and tactile limitations during freehand drilling can cause cortical perforations, especially in narrow ridges or atrophic jaws.
Pommer et al. (2011) reported a perforation rate of up to 24% in freehand implant surgeries, leading to serious complications.
Solution:
Guided implant placement, supported by digital planning services, provides a three-dimensional roadmap, significantly reducing the risk of anatomical breaches.
Perforation risks are reduced to <5% when CBCT and guides are used effectively. Surgical guides based on CBCT imaging significantly lower the chance of encroaching on thin cortical plates, especially in the anterior mandible or atrophic ridges.
5. Excessive Surgical Time and Stress
Freehand implant placement often prolongs surgical time, increases clinician fatigue, and elevates patient discomfort, especially in full-arch cases.
A study by Di Giacomo et al. (2012) demonstrated that guided surgeries consistently reduce operative time, improving overall clinical efficiency.
Solution:
By adopting All-on-X solutions with guided surgery, clinicians can streamline their workflow, reduce chair time, and enhance the surgical experience.
The Case for Guided Surgery: Precision Without Compromise
The data is clear: freehand implant placement carries inherent risks that can affect long-term success. Transitioning to guided implant workflows—using CBCT imaging, surgical guides, and digital dental design services—is no longer optional for clinicians aiming for predictable, high-quality outcomes.
At 3DDX, we offer end-to-end digital solutions, from diagnostic imaging to custom-designed surgical guides, supporting clinicians with the tools they need to minimize errors and maximize results.
Final Thoughts
Freehand implant placement belongs to a time when digital tools were unavailable. Today, clinicians have access to precise, predictable, and efficient alternatives through guided surgery.
By eliminating common freehand implant mistakes, you not only protect patient outcomes but also elevate your clinical practice to the highest standards.
Interested in enhancing your implant precision?
Discover how 3DDX’s surgical guides and digital design services can transform your workflow. Schedule a consultation with us today!
References
- Van Assche N, et al. Accuracy of computer-aided implant placement. Int J Oral Maxillofac Implants. 2012;27(2):458-64.
- Bornstein MM, et al. Accuracy of implant placement after freehand surgery. Clin Oral Implants Res. 2014;25(3):257-262.
- D’haese J, et al. Accuracy and complications using surgical guides. Clin Implant Dent Relat Res. 2012;14(2):196-203.
- Pommer B, et al. Lingual bone perforation during implant placement. Clin Oral Implants Res. 2011;22(5):557-563.
- Di Giacomo GA, et al. Computer-guided implant surgery: surgical time efficiency. Implant Dent. 2012;21(4):299-305.